This article was published earlier in CalPlanner, Volume 20, Issue 1, June 2020
By Diana Benitez and Jessica Medina, June 2020
Pandemic call to action
CALIFORNIA WAS THE FIRST STATE to enact shelter in place orders in response to the coronavirus pandemic, calling for jurisdictions to immediately implement drastic public health policies and practices. Historically, California has other firsts in the public health and planning fields, one important example being the Planning for Healthy Communities Act (SB1000). As planners with a solid understanding of the social determinants of health and the role of planning in shaping these conditions, we see SB1000 as an important step forward.
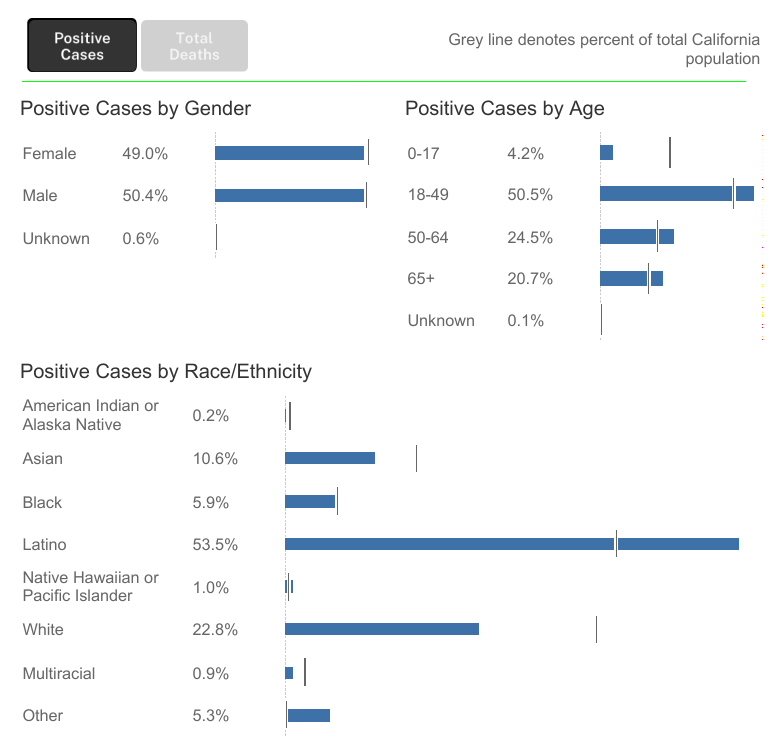
Despite California’s history of progressive approaches to health, our state has been hit hard by the pandemic. Most troubling is that our numbers tell a well-known story of health outcome disparities for people of color, particularly for Blacks, Latinos, and Native Hawaiian/Pacific Islanders, who are experiencing both a disproportionate rate of incidence and rate of mortality.
The Covid-19 experience will affect communities and planning for decades to come and this is why we are collaborating with Planners4Health California on Planning + Health in the Time of Covid-19, a webinar series and call to action.
Protecting community health today
Conversations with approximately 200 participants show us that local governments, planners, and communities are responding swiftly and with great imagination to promote physical distancing and protect community health. Compelling approaches and actions identified include:
- Cities being flexible with zoning policies to support essential businesses by easing noise restrictions and creating curbside pick-up protocols;
- Planners continuing community outreach and stakeholder engagement by going virtual, through video calls or text messaging, or back to their roots, with phone calls and mailers;
- Cities prioritizing shelter through tenant protections, opening up hotel rooms for unhoused residents, and moving forward with affordable housing development;
- Planners prioritizing streets for active transportation, recreation, and public transit for all by closing them off to vehicles, automated pedestrian crosswalk signals, eliminated fares, and continued on-demand services; and
- Cities cautiously reopening parks and beaches to enhance mental and physical health while maintaining social distance guidelines with shortened hours, active uses, and closed parking lots.
These approaches and actions protect residents from the spread of the virus, yet complicate our analysis of health equity. For example, planners are opening streets for recreation by closing them off to vehicles. The designation of these Slow Streets is done without a full consideration of whether neighborhoods want and need this response. An equity analysis would involve community input and gathering data on existing conditions and sentiments and perhaps find that some communities want to prioritize medical emergency response access, rely on vehicles for access to jobs in essential sectors, or do not feel safe in public spaces due to the over-policing and violence on Black and Brown bodies.
Promoting health equity beyond the crisis
Covid-19 has created a crisis mentality that can be paralyzing, but long-range planning is an essential service that must continue to move forward. As planners, we are concurrently responding to the crisis at hand, while keeping an eye on emerging trends and considering the future implications on cities and communities. Our thoughts at this point span across a spectrum of crisis management, trauma intervention, social resilience, land use, and application of new methodologies to build on our understanding and implementation of SB 1000:
- Making space and creating time for community members to process, grieve, and adjust to the crisis, before resuming planning activities and advocating for continued use of flexible engagement tools and practices after the pandemic;
- Learning from grassroots mutual aid efforts models that outreach to neighbors to identify physical, social, and economic needs and develop rapid response networks to address those needs;
- Upholding the health-promoting values of our public spaces and goods from sidewalks and streets to parks and beaches to air and water quality and beyond; and
- Taking advantage of the health planning tools and resources available to develop comprehensive equitable policies to mitigate future health crises.
The call to action will remain after this pandemic and we will continue to have the opportunity to rewrite the often-told story of health inequities. If we respond with intention, we can build a healthier and more equitable California.

 Diana Benitez (left) and Jessica Medina are Intermediate Planners/Designers at Raimi + Associates, working on general plans, sustainability, health, and SB 1000 implementation. Both are sheltering in place in Los Angeles and engaging others in imagining healthy futures — for example, Diana’s leadership in Planners4Health California. You can reach Diana at diana@raimiassociates.com
Diana Benitez (left) and Jessica Medina are Intermediate Planners/Designers at Raimi + Associates, working on general plans, sustainability, health, and SB 1000 implementation. Both are sheltering in place in Los Angeles and engaging others in imagining healthy futures — for example, Diana’s leadership in Planners4Health California. You can reach Diana at diana@raimiassociates.com